As a respiratory charity supporting patients throughout a global respiratory pandemic, our services have never been busier and we have never been more needed. We have also never been so hard-pressed financially to deliver our services with so few resources. Please join our asthma tribe and support us by donating now to ensure that we can continue to provide our essential one-to-one services, awareness and advocacy work to stop asthma deaths in Ireland.
More than one person dies every week in Ireland as a result of their asthma.
The feedback we get from patients and carers is that our services can be truly life-saving. Our financial situation means that we are in danger of losing some of those essential services.
Your gift to the Asthma Society can help us to survive and to keep the 380,000 people with asthma in Ireland safe.
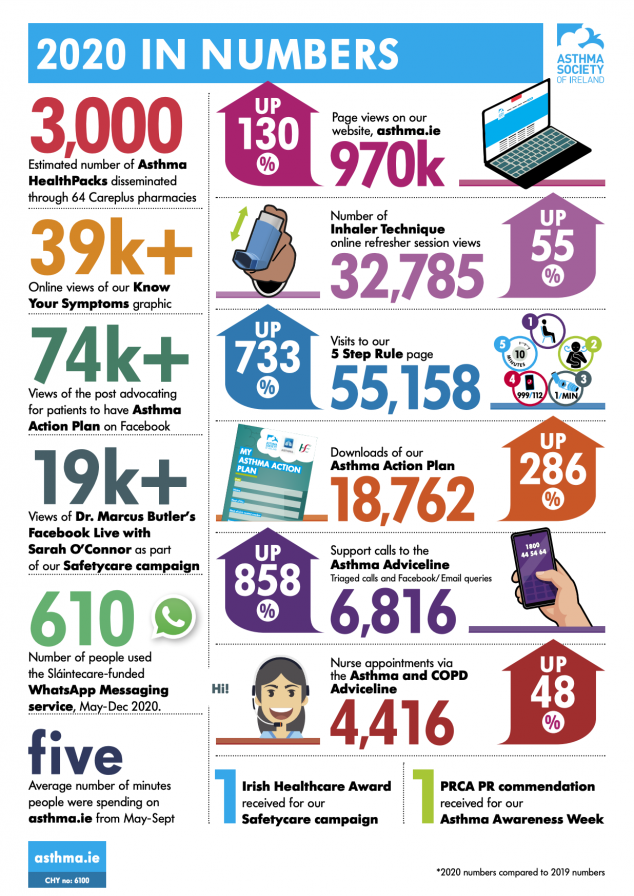
If you’d like to learn more about the scale and impact of our work, please read the 2020 Impact Assessment in Numbers below, also available as a PDF.
Copyright © Asthma Society of Ireland

The Scheme to Support National Organisations is funded by the Government of Ireland through the Department of Rural and Community Development.